
Enteroscopy
What is an enteroscopy?
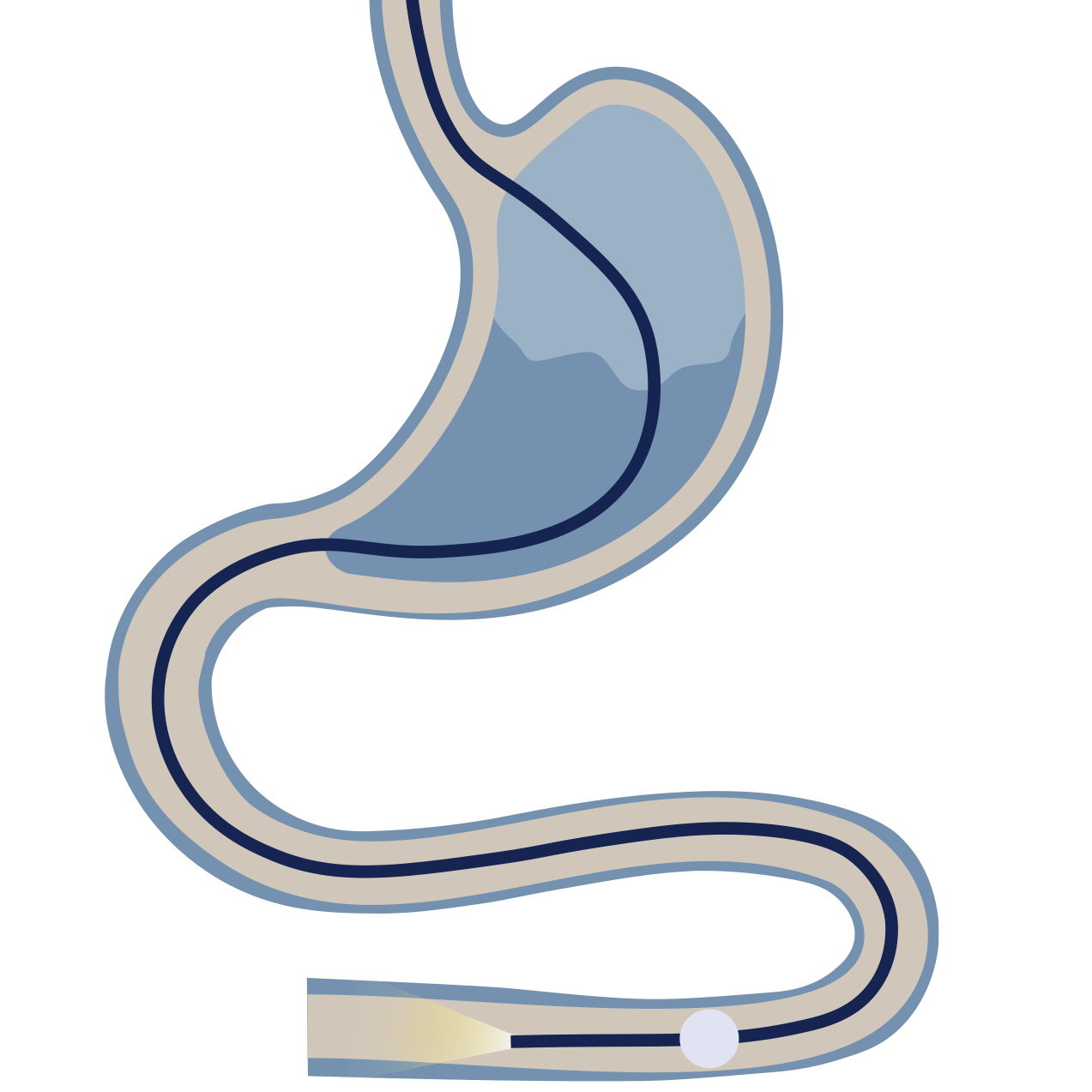
Enteroscopy is a specialised endoscopic procedure used to examine the small intestine, which is typically beyond the reach of a standard gastroscopy (which reaches the first part of the small bowel) and colonoscopy (which reaches the last part of the small bowel).
This involves using a specialised endoscope and an overtube with one or two balloons. Inflation and deflation of the balloons, combined with advancing the scope, "pleats" the small bowel over the scope, allowing it to be advanced deep into the mid-gut.
Why might you need an enteroscopy?
Enteroscopy is typically performed when a problem is suspected in the mid-small intestine that cannot be diagnosed or treated with standard gastroscopy or colonoscopy. Generally a capsule endoscopy is performed first. Reasons for enteroscopy include:
Unexplained bleeding: Investigating obscure gastrointestinal bleeding when gastroscopy and colonoscopy are normal (e.g., small bowel ulcers or vascular lesions).
Small bowel lesions: Identifying and taking biopsies or removing polyps/tumours in the small intestine.
Stricture/narrowing: Diagnosing or dilating strictures in the small bowel, often related to Crohn's disease.
Retrieval: Removing foreign objects or retrieving a retained capsule endoscope.
Assessment of Crohn's disease: Determining the extent and activity of Crohn's disease in the small bowel.
Preparing for your enteroscopy?
Preparation depends on which part of the small bowel is being examined (approach).
Upper (antegrade) approach: Requires fasting for 6 hours, similar to a gastroscopy.
Lower (retrograde) approach: Requires a full bowel preparation, similar to a colonoscopy.
Medication: You will be advised on managing blood-thinning medications if therapeutic intervention is anticipated.
What to expect?
The procedure is significantly longer than standard endoscopy, typically taking 1-3 hours. It is performed by Dr Selvanderan in the endoscopy suite.
Sedation: Depending on procedure length and complexity, deep intravenous sedation or a general anaesthetic will be administered by a specialist anaesthetist
During the procedure: The specialised endoscope is advanced deep into the small intestine using the balloon technique. Once the target area is reached, visual inspection, biopsy, or therapeutic intervention (e.g., cauterisation of bleeding sites, polyp removal) is performed.
Recovery
You will be monitored in a recovery area.
Discharge: You will usually be ready to go home within 1-2 hours after the procedure.
Post-sedation: You must not drive or operate machinery for the rest of the day. A responsible adult must escort you home and stay with you.
Bloating and gas: You may feel bloated or pass wind frequently as the gas used during the procedure leaves your system.
Results: Dr Selvanderan will discuss the preliminary findings with you before you leave. A procedure report will be sent to your referring doctor. Biopsy results typically take several days and will be communicated to you and your referring doctor subsequently. Where required, a follow-up consultation will be arranged by Dr Selvanderan’s rooms.
Risks
The risks of enteroscopy are slightly higher than standard endoscopy due to the extended time and depth of examination.
Bleeding: Risk is increased if therapeutic procedures (e.g., cauterisation, polyp removal) are performed.
Perforation: A small risk of tearing the bowel wall (rare).
Pancreatitis: A very small risk if the scope advances into the area near the pancreatic opening.
Reaction to sedation/anaesthesia: Risks associated with the sedative medication.

Expert treatment and answers with enteroscopy
Dr Shane Selvanderan performs expert diagnostic and therapeutic enteroscopy, which are critical for the investigation and management of small bowel conditions.