
Endoscopic Mucosal Resection (EMR)
What is an endoscopic mucosal resection (EMR)?
Endoscopic mucosal resection (EMR) is an advanced, minimally invasive technique used to remove large, non-cancerous (precancerous) polyps, superficial cancers, or other lesions from the inner lining (mucosa) of the gastrointestinal tract, most commonly in the colon, but also in the oesophagus and stomach.
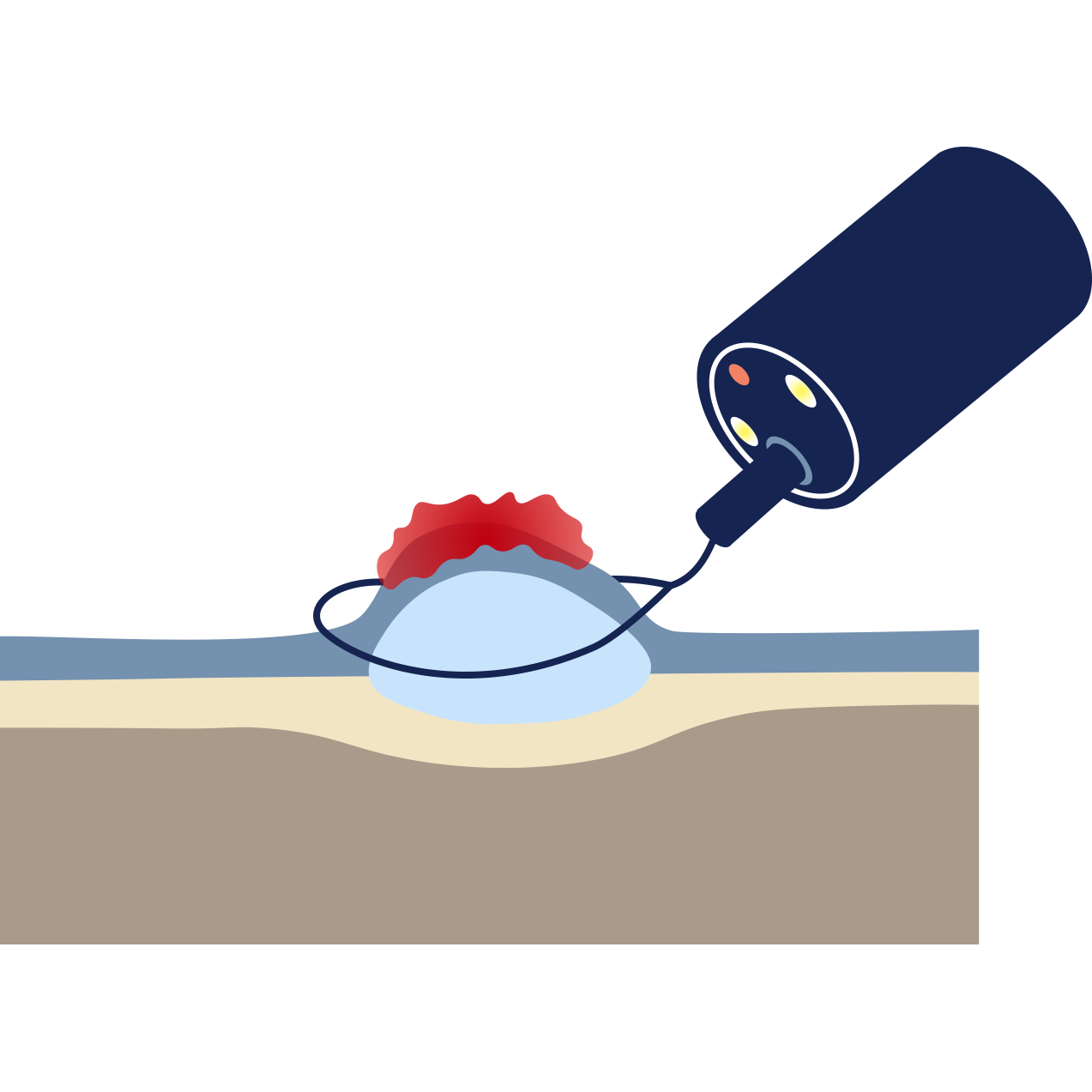
EMR is performed during a standard endoscopy (colonoscopy or gastroscopy). It involves injecting fluid beneath the lesion to lift it away from the deeper muscle layer, allowing Dr Selvanderan to safely snare and remove the tissue with a margin, often in multiple pieces (piecemeal EMR).
Why might you need an EMR?
EMR is used to remove lesions that are too large or too difficult to remove safely with standard snare polypectomy. Reasons to perform EMR include:
Large colonic polyps: Removal of large, sessile (flat) polyps in the colon, which are at high risk of becoming cancerous.
Early gastrointestinal cancer: Curing superficial cancers (e.g., early T1 mucosal cancer) that have a very low risk of lymph node spread.
Large Barrett's oesophagus Lesions: Removing high-grade dysplasia or early cancer associated with Barrett's oesophagus.
Duodenal or gastric lesions: Removal of large lesions in the stomach or duodenum.
Preparing for your EMR?
Bowel Preparation (for colon EMR): Full, excellent bowel preparation is essential to ensure a clear view.
Fasting: You must follow standard fasting instructions (typically 6 hours).
Medication: Generally blood thinning medications need to be stopped prior to EMR due to risk of post-procedure bleeding. Specific instructions will be provided.
What to expect?
EMR is performed by Dr Selvanderan during a colonoscopy or gastroscopy and typically takes between 30 and 60 minutes, depending on the complexity of the situation
Sedation: Depending on procedure length and complexity, deep intravenous sedation or a general anaesthetic will be administered by a specialist anaesthetist
During the procedure: The lesion is identified. Fluid is injected beneath it (submucosal injection). A snare is used to capture the lifted tissue, and high-frequency electric current is applied to cut and cauterise the tissue, removing the lesion. Clips are often placed at the resection site to reduce the risk of bleeding or perforation.
Recovery
You will be monitored in a recovery area until the effects of the sedation wear off.
Discharge: You will usually be ready to go home within 1-2 hours after the procedure.
Post-sedation: You must not drive or operate machinery for the rest of the day. A responsible adult must escort you home and stay with you.
Results: Dr Selvanderan will discuss the outcome of the procedure before you leave. A procedure report will be sent to your referring doctor. Pathology from the removed tissue typically take several days to be reported and will be communicated to you and your referring doctor subsequently. Where required, a follow-up consultation will be arranged by Dr Selvanderan’s rooms.
Risks
EMR is a safe and effective technique, but involves higher risks than simple biopsy.
Delayed Bleeding: The most common complication, which can occur up to 1-2 weeks post-procedure, sometimes requiring a repeat endoscopy for management.
Perforation: A tear in the bowel wall
Post-polypectomy Syndrome: Localised inflammation after a large resection (rare).
Stricture: Narrowing at the site of a large resection.

EMR in expert hands
Dr Shane Selvanderan has extensive training in advanced therapeutic endoscopy, specialising in endoscopic mucosal resection (EMR) for the safe and effective, minimally invasive removal of large and complex precancerous polyps, often avoiding the need for surgical intervention.